Center for Communications, Health and the Environment

New WHO Report Projects Hope and Help in Global Tobacco Offensive
What if we could save the lives of more than 5 million people every year?
We can...Simply by reducing tobacco use, which takes that many annually worldwide.
 |
This new WHO report details the global response to tobacco and its regulation. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
So emphasizes the WHO Report on the Global Tobacco Epidemic, 2011, the third in a series of periodic World Health Organization (WHO) assessments on the status of the global tobacco scourge and measures to curtail it.
Subtitled “Warning about the dangers of tobacco,” the report posits that tobacco knows – and shows – no mercy. The world’s most lethal consumer product, it was responsible for 100 million preventable deaths during the 20th century, WHO asserts; and left unheeded, it could kill up to 1 billion people worldwide over the course of the 21st.
Most of the millions who die tobacco-related deaths each year are working-age adults who are users or ex-users, but 17 percent – a substantial 600,000 people – are non-users condemned via second-hand smoke. Meanwhile, tobacco use is the second-biggest contributor to the global surge of noncommunicable diseases such as heart attack, stroke, cancer and emphysema, and children of pregnant smokers risk as much as a 20 percent higher chance of heart disease and stroke during their lifetimes, according to a University of Sydney study released in summer 2011.
Tobacco use and impact is growing fastest in low- and middle-income countries, due to population growth and tobacco industry targeting. By 2030, more than 80 percent of the world’s predicted 8 million tobacco-related deaths will be in these countries. At the same time, tobacco’s devastating economic and health consequences contribute to the burden of poverty in these nations, making tobacco control both a public health priority and a significant development issue, according to WHO.
While the path to preventable tobacco-related mortality is decidedly clear, trailblazing a new course is undeniably difficult and opaque. Today’s tobacco-control programs tend to operate on their own, in self-contained local, regional or national “vacuums,” and are no match for the brute force of the global tobacco epidemic, and the formidable power, reach and resources of the transnational tobacco industry. Meanwhile, traditional public health methods for reducing tobacco use, such as individual interventions by health-care professionals, are proving ineffective.
Going forward, the goal is to globalize tobacco-control approaches and initiatives to capitalize on the influence of a universally standard, united and informed front. Actions are underway to make this happen, from the unprecedented WHO Framework Convention on Tobacco Control (FCTC) to developments in countries like Venezuela, where an Intergovernmental Commission for Tobacco Control has been created to coordinate tobacco-control programs across all arms of government and to work closely with regional and international organizations.
The Promise of MPOWER
The WHO Report on the Global Tobacco Epidemic, 2011 details such successes, including policies and actions that deliver a global response to this worldwide public health problem.
The report champions the WHO FCTC, a “new approach in international health cooperation” and legally binding global treaty that provides necessary tobacco-control tools and “a comprehensive direction for implementing tobacco control policy at all levels of government” to reduce tobacco use and save lives. Adopted in 2003 in response to the globalization of the tobacco epidemic, as of January 2012, the WHO FCTC has 174 parties covering 87 percent of the world’s population, making it one of the most rapidly embraced treaties in United Nations history.
To help countries fulfill their WHO FCTC obligations, in 2008, WHO unveiled MPOWER, a package of six proven tobacco-control measures that urge nations to:
Monitor tobacco use and prevention policies
Protect people from tobacco smoke
Offer help to quit tobacco use
Warn about the dangers of tobacco
Enforce bans on tobacco advertising, promotion and sponsorship
Raise taxes on tobacco.
The 2011 WHO report examines the impact of the MPOWER measures and the progress that continues to be made in applying them globally and nationally.
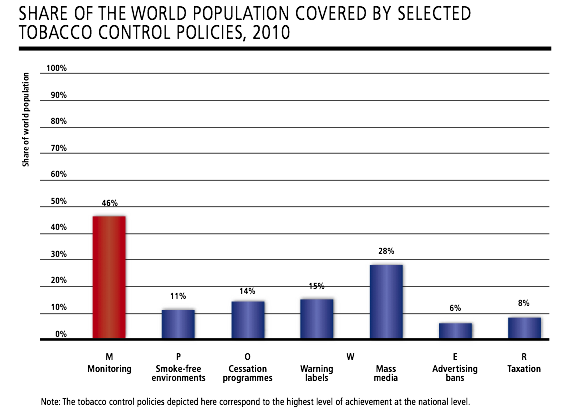 |
(Source: WHO report on the Global Tobacco Epidemic, 2011) |
“Gains were made in all areas” over the past two years, the report reveals, and roughly 3.8 billion people – 55 percent of the world’s population – are now covered by at least one MPOWER measure at the highest level of achievement, including 1.1 billion people covered by new policies in the 30 countries that enacted them since 2008. Meanwhile, more than 1 billion people (17 percent of the world’s population) live in countries that have adopted two or more MPOWER measures at the highest level.
Warning Labels Proliferate
As its subtitle suggests, the 2011 WHO report places particular emphasis on alerting people to the dangers of tobacco through such methods as large, graphic health warnings on tobacco packages and anti-tobacco mass media campaigns – two primary, cost-effective health alert strategies proven to promote awareness of tobacco’s harmful effects, reduce tobacco use and save lives.
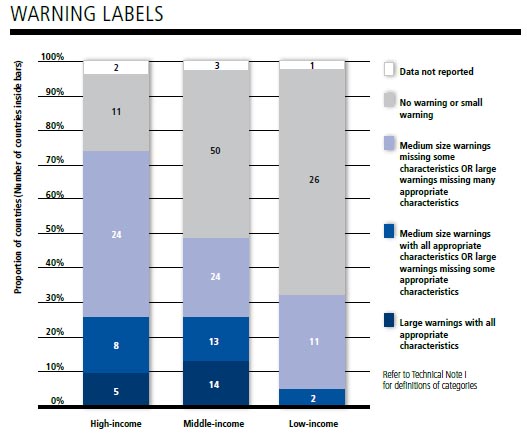 |
Warning labels make a difference and are gaining traction across the globe. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
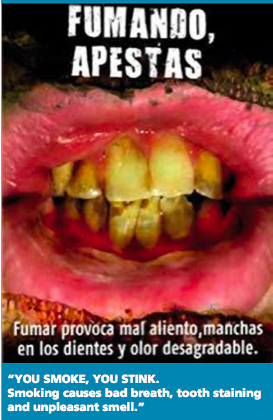
According to the report, the provision of health warning labels accounted for one of the greatest gains based on population coverage in the areas of tobacco control over the past two years, as three more countries with nearly half a billion people (Mexico, Peru and the United States) enacted pack labeling laws at the best-practice level. Today, 15 percent of the world’s population – more than 1 billon people in 19 countries – are covered by this policy, a 7 percent increase in the number of people worldwide exposed to strong graphic health warnings since 2008. And several countries have taken big steps, with commensurate impact.
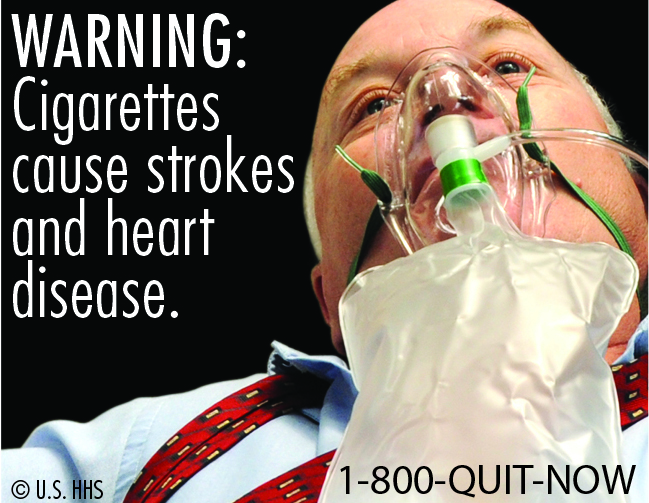 |
| New U.S. warning labels, such as the one above, are hard-hitting, but may never make it onto cigarette packs due to legal action. |
In 2009, for example, Uruguay increased the size of its graphic warning labels from 50 to 80 percent of primary pack surface areas, a bold move that resulted in nearly half of the country’s smokers considering quitting, according to findings from the Global Adult Tobacco survey. That same year, Djibouti mandated pictorial labels covering 50 percent of both the front and back of packages, and health messages on the sides; within the first year, sales of tobacco products incorporating “strong” images on warning labels were substantially lower than sales of products containing “softer” images. Attempting to follow in these nations’ sizable footsteps, the United States is slated to move from very weak warning label requirements to among the world’s strongest in September 2012, but is now facing indefinite delays due to legal action by a number of cigarette companies. (See “In the Spotlight.”) Meanwhile, only seven countries (Chile, Egypt, Iran, Mexico, Panama, Peru and Uruguay) have adopted the strongest level of regulations for smokeless tobacco warnings, including warning labels that cover at least 50 percent of the packaging.
Campaigns and Cessation
Together, health warning labels and anti-tobacco mass media campaigns are the most widely embraced MPOWER measures, based on population coverage.
Assessed for the first time by WHO in the 2011 report, comprehensive national mass media campaigns were conducted in 23 countries covering 1.9 billion people, or 28 percent of the world’s population. Able to reach large populations quickly and efficiently, often as part of a national tobacco-control program, such campaigns traditionally have relied on television’s powerful graphic imagery, but social media is increasing in importance.
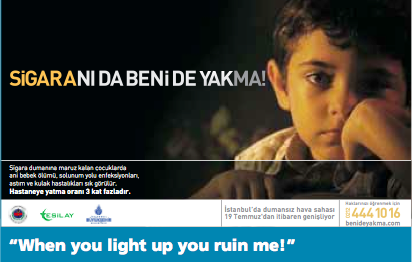 |
| This poster is part of Turkey's move to mandate more free airtime for anti-tobacco advertising. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
Currently, Turkey, which has mandated a minimum of 90 minutes of free air time every month for anti-tobacco educational programming and advertising since 1996, now requires radio and television stations to broadcast such programming during daytime, primetime and early evening hours so that messaging will reach increased numbers of adults and be more likely seen by children. And the Government of India, which allocates approximately US$5 million annually to anti-tobacco mass media campaigns, recently used its resources to run a year-long graphic, multi-dialectal, multi-phase campaign to warn the public about the dangers of smokeless tobacco. Generating press coverage and national awareness, the campaign aired hard-hitting footage of patients with tobacco-related cancers and vivid descriptions by respected physicians on television and radio; it also employed a Web site and innovative mobile technology, including text messaging, as advocacy platforms.
 |
New Zealand offers a wide range of free cessation services, including a national, government-funded quit line that assists more than 50,000 people a year. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
With warning labels and mass media campaigns fueling awareness and health concerns, tobacco dependence treatment and cessation services have increased in significance. Between 2008 and 2010, one additional country, Turkey, began providing comprehensive tobacco dependence treatment that includes a national quit line and coverage of costs for nicotine replacement therapy. Now, 19 countries comprising 980 million people (about 14 percent of the world’s population) provide the highest level of tobacco-cessation services, an increase of 76 million individuals since 2008.
According to the 2011 WHO report, high-income countries, like New Zealand, which offers a wide range of free cessation services and has subsequently seen adult smoking prevalence drop about one-third over two decades to 21 percent in 2009, were most likely to provide and fund a full range of cessation services, although less than 30 percent of countries in this income classification currently do so. Meanwhile, no low-income country yet offers a national quit line or cost-covered cessation services, and only one in eight currently covers any costs of cessation services.
Breathe No Evil, See No Evil
Other great gains made in the tobacco-control arena over the past two years involve protecting people through smoke-free environments, with the share of the world’s population covered by this policy more than doubling, from 5 percent, or 354 million people, in 2008, to almost 11 percent, or 739 million, in 2010.
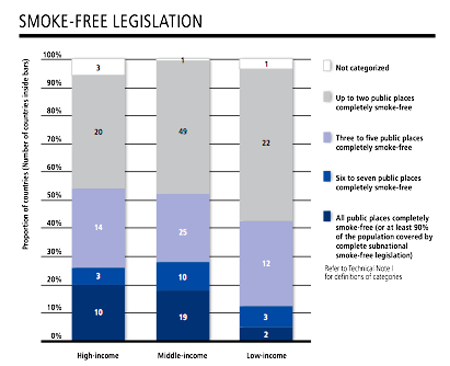 |
Making public places smoke-free is gaining in popularity. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
National-level smoke-free laws covering all public places and workplaces are popular with the public, finds the 2011 WHO report, and were newly enacted by 16 countries since 2008, increasing to 31 the number of nations that provide the highest level of protection against exposure to second-hand tobacco smoke (which increases the risk of coronary heart disease by 25 to 30 percent in non-smokers, according to the U.S. National Academy of Sciences’ Institute of Medicine). An additional 100 million people are also now protected by comprehensive smoke-free legislation at the subnational level, bringing that total to 210 million, or 3 percent of the world’s population.
Notable gains were made in Brazil, which now protects 77 million people (representing nearly 40 percent of its population) by subnational smoke-free laws passed since 2008, and in the United States, which added 21 million more people at the subnational level, the report details. Meanwhile, the Seychelles’ Tobacco Control Act of August 2009 created completely smoke-free environments in all enclosed public places and workplaces, on all transport, and in select outdoor premises, including all health and educational facilities and stadiums, continuing this nation’s pivotal role in tobacco control, including being the first country in the African Region to ratify the WHO FCTC.
 |
| Because of strong laws in the Seychelles, enclosed public spaces and workplaces, as well as all public transport, are completely smoke-free. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
The Seychelles also have completely banned tobacco advertising, promotion and sponsorship, including all forms of direct and indirect advertising, a move that, independent of other tobacco-control interventions, could decrease tobacco consumption by about 7 percent and as much as 16 percent, according to the 2009 WHO report on the global tobacco epidemic.
Currently, 19 countries with 425 million people, representing 6 percent of the world’s population, are fully protected against tobacco industry marketing tactics, 80 million more than in 2008 owing to the comprehensive bans enacted by Chad, Colombia and Syria over the past two years, reveals 2011 WHO report data. Of these 19 nations, nine are classified as middle-income, six as low-income, and four as high-income, with Norway the only country in Europe and North America to enact and enforce a complete ban on all forms of direct and indirect tobacco advertising. An additional 101 countries throughout the world ban national television, radio and print tobacco advertising, as well as some other forms of direct and/or indirect advertising, but studies reveal that partial bans such as these have little or no effect. Meanwhile, 74 countries, or 38 percent of all nations, currently do not have any restrictions on tobacco advertising, promotion and sponsorship, or have very minimal ones.
Tracking and Taxes
On the brighter side, the recent WHO report finds that 3.2 billion people in 59 countries – 46 percent of the world’s population – are covered by high-level monitoring policies, which form the backbone of tobacco-control efforts and provide the accurate data necessary for their success. Between 2008 and 2010, 23 additional countries strengthened their tobacco use monitoring to include recent and representative data for both adults and youth, and also conducted ongoing periodic surveys that collect these data at least every five years. Despite such progress, however, more than 100 countries lack representative data for adults and youth, or have no data at all – and an additional 30 countries do not have periodic data, making it difficult to accurately track tobacco-use trends.
Monitoring provides the foundation for effective tobacco control, but “[i]ncreasing taxes is the best way to reduce tobacco use,” contends the 2011 WHO report. In fact, according to 2008 WHO MPOWER data, each 10 percent increase in retail price reduces consumption by about 4 percent in high-income countries and up to 8 percent in low- and middle-income countries, with smoking prevalence reduced by about half those rates. Based on the new WHO tobacco report, 539 million people in 26 countries and one territory, including Argentina, Latvia and the West Bank and Gaza strip, now have taxes constituting the recommended minimum of 75 percent of retail price, an additional 115 million people than in 2008. Only one low-income country, Madagascar, and less than 10 percent of middle-income countries currently levy taxes at this recommended level, and six countries that had taxed tobacco at that level in 2008 saw their share of taxes as a proportion of retail price fall below the 75 percent benchmark by 2010. In a somewhat surprising move, Japan, a country with relatively few anti-smoking laws, levied that country’s biggest cigarette tax increase in October 2010, raising prices nearly 40 percent in a move designed to be both a public health initiative and a source of tax revenue for the government.
At the same time, governments in general are falling short in their funding of tobacco-control activities. In fact, governments collect nearly US$133 billion in tobacco excise tax revenues, but spend less than US$1 billion combined on tobacco control, with 97 percent of this amount spent by high-income countries, details the 2011 WHO report. Yet, WHO asserts, adequate resources, including sufficient staffing, are critical to the success of tobacco-control interventions, most of which are carried out locally but depend on higher-level assistance.
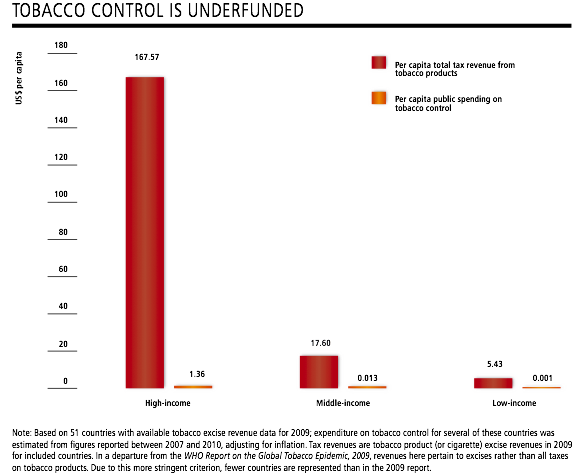 |
(Source: WHO Report on the Global Tobacco Epidemic, 2011) |
“To Great Effect”
Programming and policy are important components of reducing tobacco use across the globe. But it is national action, supported by civil society and a global vision, that is imperative and makes a difference on a mass scale.
Most countries have developed tobacco-control programs or strategies, but only 20 percent of high-income countries and 24 percent of middle- and low-income countries have an agency with at least five full-time equivalent staff members – and just three countries (Burundi, Pakistan and Turkey) increased program staffing to this level in the past two years, reveals 2011 report data. Meanwhile, another 30+ countries either do not have a national tobacco-control agency or have not established national objectives for tobacco control, which are critical foundations for complying with WHO FCTC treaty obligations.
 |
Some smaller countries stand out as tobacco-control role models, like Uruguay, which has the world’s largest pictorial health warning requirements for cigarette packages at 80 percent. (Source: WHO Report on the Global Tobacco Epidemic, 2011) |
Nevertheless, “The status of the MPOWER measures presented in this WHO Report on the Global Tobacco Epidemic, 2011 show that it is possible for any country, regardless of political structure or income level, to implement an effective tobacco control programme to reduce tobacco use,” emphasize the authors of the report. Within the past year, for example, the Russian Federation adopted its Concept for State Policy on Actions Against Tobacco use for 2010–2015. This plan establishes a formal tobacco-control operation within the country’s Ministry of Health and Social Development with responsibility for implementing a comprehensive national strategy that addresses all WHO FCTC requirements, including provisions on tax increases, advertising bans, smoke-free places, warning labels, cessation services and public education activities; it also sets specific program goals for 2015 such as reducing tobacco use prevalence by 10 to 15 percent and halving the number of people exposed to second-hand tobacco smoke.
Many other, smaller, developing countries have taken significant steps to combat tobacco use and can be looked to as MPOWER role models. Case in point: The three countries that currently have the largest pictorial health warning requirements for cigarette packages (as an average of the package front and back) are Uruguay with 80 percent, and Mauritius and Mexico with 65 percent.
“The progress in reaching the highest level of the MPOWER measures is a sign of the growing success of the WHO FCTC and provides strong evidence that there is political will for tobacco control on both national and global levels, which can be harnessed to great effect,” concludes the 2011 WHO report.
To “great effect” indeed – millions more lives could be saved and hundreds of billions of dollars a year in avoidable health-care costs and productivity losses averted. But such a considerable impact requires countries to continue to expand and intensify their tobacco-control efforts, ensuring that they have the financial means and political commitment to support effective and sustainable programs, and, most importantly, can transform these dollars and dedication into human action and realizable results.
Read More:
Spotlight Article: New Graphic Warnings Could Have Great Impact - IF Enacted
Also Noted: E-Cigs Come Under Scrutiny
CECHE News: CECHE Champions Tobacco Control and Intervention Programs Around the World

Dr. Sushma Palmer, Program Director
Valeska Stupak, Editor & Design Consultant
Shiraz Mahyera, Systems Manager
Daniel Hollingsworth, Website Consultant