Center for Communications, Health and the Environment

Obesity and Overnutrition Trump Undernutrition in Newly Affluent Nations
Fatness was once a sign of power, prestige and beauty worldwide. Consider King Henry VIII, Fat Men’s Clubs and their well-to-do “fat cat” members, 200-pound “American beauty” and stage star Lillian Russell, and even the 13th century Mongol ruler and founder of the Yuan Dynasty, Kublai Khan.
To be fat communicated prosperity and success, especially in countries historically prone to food shortages and famine, such as China and India. But until the past half-century, most Chinese and Indians were slim, either because they were engaged in physically demanding professions, or because they were impoverished and undernourished.
The Epidemic Is Global
The 21st century, however, is characterized by a global obesity epidemic. While about 850 million individuals around the globe battle undernutrition and almost 16,000 children die from hunger-related causes every day, more than 2 billion adults worldwide are overweight or obese, according to the latest World Health Organization (WHO) data. A growing number of children – at least 20 million – are also confronting obesity, which may place them at risk of a shorter life expectancy than their parents.
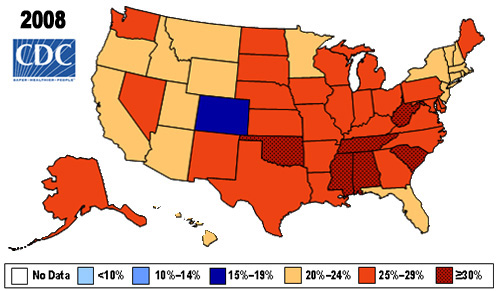
In a study published in the July 2008 issue of Obesity, researchers at the Johns Hopkins Bloomberg School of Public Health conclude that unless eating or exercise habits change, 86 percent of the American population will be overweight or obese by 2030. Meanwhile, more than a third of American adults – over 72 million people – were already obese in 2005 and 2006, according to the Centers for Disease Control and Prevention (CDC).
 |
But America is not alone. “[A]ll of a sudden we're seeing the same problems in places where 20 years ago all they worried about was hunger: in Egypt, and among blacks in South Africa, and in China, where a third of adults now are overweight and obese,” points out Barry Popkin, professor of global nutrition at the University of North Carolina at Chapel Hill, in a December 2008 Newsweek Web interview. “In Mexico, nobody was overweight 15 years ago; now 71 percent of Mexican women and 66 percent of men are.”
According to experts across the globe, the world’s obesity epidemic stems from a major shift in diet over the past century from primarily cereals to substantially animal products and fats, as well as an overall increased caloric intake, accompanied by a decline in physical work and activity precipitated by urbanization, and the rise and ubiquitousness of technology, motorized transportation and sedentary leisure activities, such as television viewing. In short, we are embracing less healthy food and more sedentary lifestyles.
China Is A Prime Example
 |
Take China, for example. Plumpness was seen as a sign of prosperity, health and harmony with the spiritual world; it was celebrated, and sought, reports James L. Watson, Fairbank professor of Chinese Society and professor of Anthropology at Harvard University, in “Prosperity versus Pathology: A social history of obesity in China.”
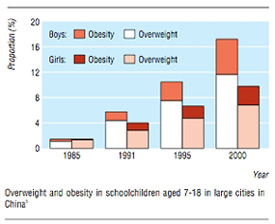
Obesity remained at bay, however, until the late 1980s, when, Watson notes, “the dietary implications of rising affluence” weighed in and nutritionists like Georgia Gulden at the Chinese University of Hong Kong began to note unsettling trends: She recorded obesity rates exceeding 20 percent among certain subsets of male children in Beijing in 1995 and of 21 percent among Hong Kong 11-year-olds in the mid-1990s. From the cabbage subsistence days of socialism, in just two decades (beginning with Deng Xiaoping’s reforms in 1978), “China moved from a diet rich in grains and vegetables to one laden with red meat, sugar and edible oils,” Watson explains. Meanwhile, in Hong Kong, Shanghai and Taipei, the advent of convenience foods, take-out cuisine and food-on-demand has skyrocketed.
 |
Popkin concurs. “Up until three years ago, there was no snacking in China,” he explains in his December 2008 interview. “Now it's exploding...Because all of a sudden, there are Chinese equivalents of Wal-Mart...[and] supermarkets everywhere, and everybody sees the same TV we see and wants the same things we want.” Meanwhile, “...people in the rural areas are as fat or fatter than they are in the urban areas,” due to the advent of “cheap food” and the replacement of physical labor with machines such as tractors, Popkin notes, citing both China and Mexico as examples.
Interestingly, studies show that, while being a little chubby may slightly increase life expectancy, being overweight or obese is a definitive, and serious, health risk. According to data in a January 2009 Student BMJ article and the 2007 Textbook of Men's Health and Aging, approximately 80 percent of obese adults have at least one, and 40 percent have two, or more associated diseases such as diabetes, hypertension, cardiovascular disease, gallbladder disease and cancers.
Developing Countries Set to Suffer Most
The increase in obesity-related complications continues to be most noticeable in developing countries. In nations like China, at least 25 percent of the population currently is overweight or obese, and according to WHO statistics, hypertension increased 12 percent (or the equivalent of 160 million people) between 1991 and 2002. Meanwhile, WHO predicts that three-fourths of the more than 350 million diabetics projected in 2025 will inhabit the third world, and that diabetes deaths will increase by more than 50 percent worldwide by 2016.
According to the U.S. Department of Agriculture (USDA) September 2008 Amber Waves Internet Edition article “Obesity in the Midst of Unyielding Food Insecurity in Developing Countries,” already “an estimated 25-50 percent of the population in countries like Mexico, Thailand, and Tunisia suffer from diabetes,” and rates are surging in China.
But it is India that has the largest number of diabetics, both diagnosed and undiagnosed. Data from the Diabetes Atlas, Third Edition reveal that, in 2007, India had 40.9 million diabetics age 20 to 79 – double America’s 19.2 million and more than any other country in the world. (China ranked second with 39.8 million.)
Expected to reach a staggering 70 million by 2025, India’s diabetic population illustrates the projection that the developing world will bear the brunt of the rising obesity burden. Genetically vulnerable to diabetes and contracting it at an earlier age then people in developed countries, many middle-class Indians in particular confront both diabetes and obesity, and spend more than a quarter of their incomes to pay for diabetic treatments because of India’s dearth of medical insurance.
India is a prime example of the swift changes and stark dichotomy faced by many developing countries in the wake of the global tidal wave of obesity-promoting lifestyles, foodstuffs and behaviors. The country’s newly wealthy, urban middle class is adopting Western ways – and the resultant increase in body weight and noncommunicable disease burden associated with them – at the same time that the country is battling the malnutrition of millions in its impoverished rural regions. So, while around 45 percent of Indian children under five suffer from malnutrition, according to the World Bank, nearly half of India’s 250 million adolescents are overweight and 66 percent of women in New Delhi suffer from abdominal obesity, reveals a recent pan-India survey by the All-India Institute of Medical Sciences. In fact, the country that has more undernourished people than any other nation in the world also has one of the globe’s highest McDonald’s service volume averages, delivering fare to 13,000 customers per minute at outlets across India, reports Malaysia’s StarWeekend in a November 2008 article, “Rising obesity in India.”
How and Why Do Obesity and Undernutrition Coexist?
According to the September 2008 Amber Waves article, “The answer lies mainly in differences in income levels among and within countries,” and the resulting gross disparity in purchasing power, food choice, food consumption and lifestyle options.
 |
The “Food Security Assessment, 2007,” conducted by the USDA’s Economic Research Service, reveals that people in the lowest income quintile of a country tend to hold significantly less of that nation’s total income than those in the highest quintile. These poorer individuals eat accordingly, generally consuming less than the daily nutritional requirement, while those in the highest quintile exceed the requirement, sometimes by as much as 30 percent.
Meanwhile, and especially marked in the higher income groups, “Average per capita food consumption in developing countries increased 28 percent between 1970 and 2005, three times the rate in developed countries.” At the same time, per capita income in developing countries nearly tripled during the period, the Amber Waves article notes, precipitating a shift toward increased calorie intake and the consumption of fattier and more processed foods, particularly in money-infused, urbanized behemoths like China, Brazil and India.
And although real food prices have increased over the past five years, they declined from 1970 until 2004, report Stacey Rosen and Shahla Shapouri in Amber Waves. This may explain why, between 1970 and 2005, per capita consumption of “...meat, eggs, and vegetable oils increased roughly threefold, while sugar increased 66 percent.”
 |
Developing countries with the highest number of urban dwellers tend to maintain higher-calorie diets – and higher obesity rates. According to Chinese Academy of Medical Sciences’ Dr. Yangfeng Wu in a 2006 BMJ editorial entitled “Overweight and obesity in China,” data from China national surveys of nutrition show that “[e]nergy intake from animal sources has increased from 8% in 1982 to 25% in 2002, and the average energy intake from dietary fat among urban Chinese increased from 25% to 35%,” exceeding the maximum 30 percent recommended by WHO. Meanwhile, in India, two of every three urban women over the age of 35 are overweight or obese, according to the newly released results of a three-year national multi-site study on nutrition and nutrition-related noncommunicable diseases funded by the country’s Department of Science and Technology.
Urban consumers are presumably the driving force behind the more than fivefold growth between 1970 and 2005 in imports to developing countries of highly processed foods such as canned meats, breakfast cereals, pastries and wine. The surge in supermarkets – which in the last 20 years have become almost as ubiquitous in the developing world as in the developed – has fueled the prevalence of such convenient, and culpable, consumables as well.
And, of course, there is culture. “The likelihood of being overweight in the poorest 25% of the population is twice that of people in the highest quarter of economic class,” states Dr. Kelly D. Brownell, co-founder and director of Yale University’s Rudd Center for Food Policy and Obesity, in a 2007 LA Times series entitled “The Great Fat Debate.” Thus, while overweight and obesity are associated with poverty and lower income groups in developed Western countries today, in developing countries such as China and India, obesity may be rooted in the age-old cultural belief that “excess body fat represents health and prosperity,” explains Wu. Bigger children are often considered evidence of affluence and success in China, for example, and with the country’s one-child rule, overweight youth are a dime a dozen, as food that used to be shared by multiple siblings prior to 1979 is now consumed by one person, observes George Washington University’s Dr. Tsung O. Cheng in a July 2008 reader’s letter on Beijing Review.com.
How to Halt the Epidemic
Just a few years ago, China was already spending about 5 percent of its gross national product (GNP) on direct and indirect costs related to poor diet, lack of physical activity and obesity, according to Popkin in the August 2006 National Geographic News article “Obesity Explosion May Weigh on China's Future.” As overweight and obesity figures there continue to skyrocket, “...it’s only a matter of time before obesity-related spending catches up to that of the United States, which spends 17 to 20 percent of its GNP on related costs,” Popkin says.
Echoing this sentiment, Student BMJ “Obesity in the developing world” authors Hannily Harvey and Janneke Patterson contend that “[i]nevitably, a reallocation in government healthcare spending will be required if any progress is to be made in halting the progression of this phenomenon. Unfortunately, in countries where economic and social resources are minimal, diverting monetary focus could lead to abandonment of the ongoing campaign against infectious disease.”
But lifestyle changes could have a major, positive impact.
In its “Facts Related to Chronic Diseases,” WHO states that up to 80 percent of cases of coronary heart disease, 90 percent of cases of type 2 diabetes and one-third of cancers could be avoided by switching to a healthier diet, increasing exercise and stopping smoking. (See www.who.int/dietphysicalactivity/publications/facts/chronic/en/print.html.)
For example, a Mediterranean diet, which is rich in vegetables and fiber with moderate amounts of red meat and fat, and a high proportion of monounsaturated fat (mostly from olive oil and nuts), provides cardiovascular benefits, according to articles in a 2006 Annals of Internal Medicine and a 2008 New England Journal of Medicine (NEJM). Other studies indicate that such a diet may be beneficial for weight loss. In addition, a two-year “Dietary Intervention Randomized Controlled Trial” published in a July 2008 NEJM found that a low-fat, restricted-calorie diet, a Mediterranean, restricted-calorie diet, and a low-carbohydrate, non–restricted-calorie diet led to mean weight loss (of 3.3 kg, 4.6 kg and 5.5 kg, respectively) and precipitated significant reductions in insulin levels in participants both with and without diabetes.
While improving diet is essential, it is not always considered – and quite often ignored. In India, for instance, the middle- and upper-income individuals who represent the bulk of the country’s obese population and who can afford to buy fruits and vegetables aren’t. They instead spend their rupees on fried, sugary, salty, obesity-generating snack foods, which are no less expensive than healthy foods, and in fact, often cost more.
Such behavior belies deeply rooted cultural norms, as well as a certain backwardness associated with a lack of awareness and education.
This is where government agencies, nongovernmental organizations, industry and educators can play an important role.
Programs and Partnerships
According to “Obesity...At A Glance 2009,” a publication of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, “[p]ublic health approaches that affect large numbers of different populations in multiple settings...are needed. Policy and environmental change initiatives that make healthy choices in nutrition and physical activity available, affordable, and easy will likely prove most effective in combating obesity.” And this is true across the globe.
The CDC itself actively develops partnerships and sponsors state-based programs, as well as national ones, like the YMCA’s extensive “Activate America: Pioneering Healthier Communities™” project, which promotes the development of effective strategies and programs for healthy living in communities across the United States. The CDC also convenes national leadership activities and is leading development of the “National Roadmap for Obesity Prevention and Control,” expected to be unveiled in 2010.
On the international front, WHO and its “Global Strategy on Diet, Physical Activity and Health” form the backbone of many a program and policy, including Britain’s multimillion-dollar “Change4Life” anti-obesity campaign, which employs media outlets, the Internet and a helpline to educate and curtail the consequences of poor diet and inactivity, and is the country’s biggest obesity-related marketing campaign to date.
|
Source: http://www.nhs.uk/change4life. Used with permission |
There are also major campaigns underway in many parts of the world to promote vegetables and fruit, or a plant-based diet. One such vigorous program is the “5-A-Day The Color Way” campaign that started in the United States in the 1990s and recently debuted in Europe. “5-A-Day” is a coalition of the U.S. National Cancer Institute, the Public Benefit Foundation, the fresh produce and agriculture industries, Wal-Mart and a host of others, including educators and media. It promotes consumption of at least five servings of vegetables and fruits each day using clever and persuasive ads, public service announcements and promotional materials for adults and children, and it has had a small, though measurable, impact in increasing vegetable and fruit consumption in the United States.
But it is in developing countries where such public health approaches are needed most – and fortunately, some are beginning to take root.
The CECHE-supported and Center for Science in the Public Interest-led “Global Dump Soda Campaign,” for example, aims to prevent obesity in children by curbing soft drink consumption, and inappropriate and aggressive marketing in less developed countries. The Indian version of the program, which involves a partnership with the consumer advocacy coalition VOICE, is even broader in scope, targeting not just soda, but all fatty, fried, and high-salt and -sugar foods.
 |
Singapore’s Holistic Health Framework (HHF) specifically addresses schoolchildren, focusing on improving physical fitness and mental and social well-being through healthy lifestyle choices. The HHF replaces the country’s 15-year ministry-managed “Trim and Fit” program, which was, according to the September 2008 Amber Waves article, “...credited as one of the most successful programs in the world in terms of sustained obesity management.” Consisting of “teacher and student education, changes in school lunches, assessment of students, and increased physical activities during school time...,” the program, which was disbanded after being criticized for “targeting overweight children and thereby stigmatizing them,” saw the percentage of students who passed the government’s national fitness test increase from less than 60 percent in 1992 to more than 80 percent in 2002, and the portion of overweight students drop from 14 percent in 1992 to 9.5 percent in 2005.
Also aiming to control obesity among schoolchildren is China’s national Health Promoting Schools project. A collaboration with WHO, the project includes more than 50 schools in 11 cities across the country’s Zhejiang Province. The schools implement interventions through a host of actions, including establishing health-related policies, improving physical environments and promoting a sense of individual responsibility for health-related behaviors and lifestyles. Based on an earlier pilot program, results have been inconsistent, with limited studies indicating everything from significant benefits in the intervention group for girls and boys after one year, effectiveness in girls only after 10 months, and the inability to effectively prevent and treat obesity after two years.
Several other obesity-related intervention programs have also been implemented in China since the 1990s with varying results. For example, Jiang, Xia, Greiner, et al conducted a two-year family-based behavior treatment program in early 2000 among 68 obese children in a Beijing middle school whose published results showed a 2.9 (or 9.8 percent) decrease in BMI and a 2.5 kg m-2 reduction, as well as a 5.5 percent dip in total cholesterol and a 9.7 percent drop in triglycerides in the treatment group. Meanwhile, two-year individualized interventions among adults, including a 2006 study on “the effect of community-based integrative intervention on hypertension in Guangzhou” and a 2001 “dietary intervention study on the hypertensive high risk population in a northern rural area of Beijing,” saw 6.8 percent of the overweight/obese subjects in the intervention group of the first program lose weight to reach a normal BMI; and the overweight rate decrease 3.5 percent in the intervention group, while rising 18 percent in the control group in the latter, rural initiative.
Action Required
By all accounts, the world has become “obesogenic.” As the above examples show, some efforts are underway to beat this global trend towards weight gain driven by the overconsumption of unwholesome foods combined with a sedentary lifestyle. However, it is apparent that, to succeed, there needs to be a massive and sustained global multi-faceted effort comprising national and local components that especially target children in schools and at home, because that is when and where food habits are formed.
Among the key components of this effort should be extensive, sustained mass media initiatives to educate the public about obesity and how to prevent it. But while the “5-A-Day” and “Change4Life” campaigns are making headway in developed countries, public education programs that target obesity in developing nations like India and China have yet to take advantage of a growing opportunity to reach the public through television and other mass media to inform and motivate them to change their lifestyles.
Also fundamental to combating obesity is controlling junk-food advertising and availability, and requiring regular physical activities at schools, á la the United Arab Emirates, where the Ministry of Education plans to ban junk food in all public and private schools across the country and will ensure that each student exercises daily for at least 30 minutes through intensive one-on-one training.
Updating decades-old school nutrition standards would also pack a punch. And currently in the United States, legislation has been proposed in the House of Representatives and the Senate to update nutrition standards for the foods sold alongside school meals in the cafeteria, as well as in vending machines and school stores, and to broaden the 1979-era standards to apply everywhere on campus during the whole school day (as opposed to only in the cafeteria during mealtimes).
Farm subsidies programs could also be restructured to favor nutrient-dense rather than calorie-packed produce. And countries, states or provinces could tax sugary and high-calorie beverages, as proposed by New York Gov. David Paterson in his January 2009 “State of the State” address, during which he asserted that an 18 percent tax on soda and other soft drinks would reduce consumption by 5 percent and raise $404 million next year to fund obesity prevention and other programs in the state. Brownell and Dr. Thomas R. Frieden also make a public policy case for taxes on sugared beverages. In their April 30, 2009 NEJM article, they present data that indicate that higher prices reduce soda consumption and that a tax on sugared beverages – even a one-penny-per-ounce excise tax – could cut consumption by more than 10 percent and encourage consumers to switch to more healthful beverages.
Legislating basic medical coverage in countries like India, where insurance is insubstantial at best, could also have profound effects. So could “mandat[ing] insurance coverage for preventing and treating pediatric obesity,” argues Dr. David S. Ludwig of Harvard Medical School and the Optimal Weight for Life Program at Children’s Hospital Boston.
No single approach is sufficient to win the fight against overweight and obesity, but beginning with even one of these initiatives would give the challenge a renewed sense of urgency and, most importantly, a chance.
It is in developing countries that we have a historic opportunity to halt, or at least minimize, the epidemic of obesity. And experience in industrialized countries tells us that this can and must be done.
Read More:
Lead Article: Obesity and Overnutrition Trump Undernutrition in Newly Affluent Nations
In the Spotlight: The Economics of Obesity
CECHE News: CECHE Promotes Healthy Hearts
Also Noted: Is Obesity Contagious?

Dr. Sushma Palmer, Program Director
Valeska Stupak, Editorial & Design Consultant
Shiraz Mahyera, Systems Manager
Daniel Hollingsworth, Website Consultant